












Why Stroke Recovery Doesn't Have To Stop At The Plateau
A look at what really happens when formal rehab ends, why so many survivors hit a wall, and how staying in motion can help keep the progress going.
For a lot of people rebuilding mobility after a stroke, the hardest moment is not the hospital. It is the day the progress seems to stop. The gains that came fast at first slow down, the therapy sessions run out, and someone quietly suggests that this might be as good as it gets.
That wall, though, is usually the end of a therapy schedule, not the end of what a body can do. This page looks at why the plateau happens, what the research actually says about recovery, and where a three-wheeled walking bike called the Alinker fits for the people it can help.
First, an honest caveat. The Alinker is not a treatment. It does not cure, reverse, or fix anything. It is a mobility tool, and what it offers is a way to keep moving and keep getting back out into the world, which for many survivors is exactly what stalls when the appointments end.
Section OneThe Overnight Change, And The Ladder Back
Most conditions arrive slowly, but a stroke does not. The most common way survivors describe it is that they went to sleep as one person and woke up as another, active and independent one day and relearning how to stand the next.
What follows is a climb that the community even talks about like a ladder, moving from a wheelchair to a walker, then to a cane, and finally to walking unassisted. Each rung feels like a promotion, and the goal at the top is almost always the same single word: independence. Regaining walking is treated as the whole prize, because walking is what carries the rest of a life with it, from the grocery run to the dog walk to the simple dignity of standing at eye level in a conversation instead of looking up from a chair.
That climb is also where the affected side becomes its own character in the story. Survivors talk about "my stroke leg" and "my affected side," about a love and hate relationship with a cane, and about the strange new fact that every step now takes conscious thought. As one survivor put it, you have to think about every step you take.
Section TwoThe Wall, And What The Research Actually Says
Somewhere between the first and third year, a lot of survivors describe the same thing. The fast early gains slow, then stall. One survivor called it hitting a brick wall, and the phrase sticks because so many people recognize it.
What causes that wall is usually not biology but the calendar. Insurance-covered therapy runs on a schedule, so when the sessions end, the daily hours of structured, repeated movement end along with them. Recovery itself does not hit a ceiling; the practice that was driving it simply stops.
The research is more hopeful than most people are told. The adult brain keeps its ability to adapt and rewire throughout life, a property scientists call neuroplasticity. Stroke rehabilitation studies have shown that structured, repeated practice of a movement can drive real gains, and that meaningful recovery can continue for months and even years after a stroke, long after many people are told they have plateaued. Clinicians even have a phrase for it: use it or lose it.
The plateau is not always the ceiling
The curve most survivors are shown rises fast, then flattens when therapy ends. Tap below to see what research suggests can happen when movement keeps going.
Illustrative concept, not a prediction of any individual result. Recovery varies from person to person.
Section ThreeHow The Alinker Keeps You Moving
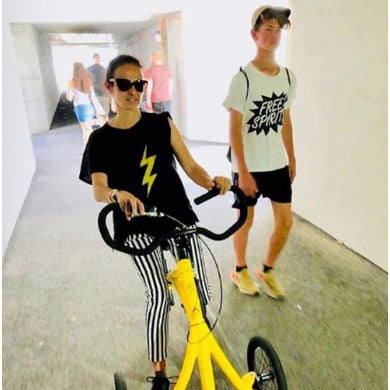
The Alinker looks like a small bicycle without pedals. It has three wheels, a saddle set at standing eye level, and handlebars at the height a cyclist would use, with no motor and nothing to pedal. You sit on the saddle, keep your feet on the ground, and walk in much the same motion you would use without it.
What the saddle does is the whole point. It carries most of your body weight, so your legs are free to keep moving without having to carry the full load. For someone with one-sided weakness, that matters in a specific way: because both feet stay on the ground and move together, your stronger side helps share the work with the affected one. You keep walking, and you keep using the leg that a stroke made harder to use.
You sit. Your feet stay on the ground. You walk, and the bike carries the part that is tired. Your strong side helps your weak side, and your eyes stay level with the world.
Because it reads as a bike rather than a medical device, it also answers something survivors bring up constantly. A cane, a walker, or a brace announces a diagnosis before you have said a word, while the Alinker, in bright yellow, does the opposite and lets people see your face first.

Section FourIs The Alinker Right For You?
The most useful thing we can do here is be honest about fit. The Alinker is not right for everyone recovering from a stroke. It needs both feet on the ground and the ability to take steps, so it suits people who have gotten some walking back, rather than people who rely on a wheelchair to get around. If that is where you are today, the quick check below will tell you plainly, and so will our team.
A quick honesty check
Four quick questions, answered honestly. This is about finding the right fit, not making a sale.
Section FiveWhat Alinker Riders Say
The Alinker has been part of daily life for thousands of riders across four continents, each with a different condition but a shared reason for riding, which is to keep moving and stay part of the world. Here are a few of them, in their own words.
I am paralyzed on my left side, so it helps me to walk for longer distances. Instead of sitting in the wheelchair and feeling a lot more disabled, this makes me feel like I am on my way to becoming healthy again. Diane, Alinker rider with left-side paralysis
It is a game changer. I can keep up with my son on a walk while activating my brain without overstressing my body. Selma Blair, actor and Alinker rider
With the Alinker I am independent again. Antonia, Alinker rider, Netherlands
The phrase that comes up more than any other, across every condition, is a simple one: riders say their world got bigger. When mobility shrinks, the world shrinks along with it, taking the block you stop walking to, the market you stop visiting, and the reasons to leave the house at all. Getting back out into that world is the whole point.
Section SixHonest Answers To The Real Questions
Tap any question for a straight answer.
For many people with one-sided weakness, yes, as long as you can still bear weight and take steps. Because both feet stay on the ground and move together, your stronger side helps carry and stabilize while your affected side keeps working. The people it does not fit are those who cannot put weight on a leg or take steps at all. The quick check earlier on this page is the fastest way to tell.
This is an honest limitation worth naming. You steer and brake with your hands, so significant weakness or tightness in the hand on your affected side can make the Alinker harder or unsafe to control. Some riders manage well with one strong hand, and others find it does not work for them, which is exactly the kind of thing our team will talk through with you before you commit.
Yes, and we are upfront about it. Most new riders describe a short adjustment period while the body gets used to the saddle and the motion. The advice from longtime riders is to keep the first few outings small: a familiar path, a friend or family member nearby. Most riders find their rhythm within the first week or two.
No. The Alinker is a mobility tool, not a medical treatment, and it does not replace your care team. It works alongside your doctor and your physical therapist. Think of it as a way to keep moving day to day, not a substitute for professional guidance. Always check with your own clinician about what is right for your recovery.
If you cannot put weight on a leg or take steps, rely on a wheelchair to get around, or have balance or awareness challenges that would make steering and braking unsafe, the Alinker is not the right tool, and we would rather tell you that now than have you end up with a bike that does not fit your life.
What An Alinker Gives You
For the riders it fits, this is what the bike delivers.
- A way to keep moving after therapy ends. When the structured hours run out, the Alinker is a way to keep walking, at your own pace, every day.
- Your strong side helps your weak side. Both feet stay on the ground and move together, so the stronger leg shares the work while the affected one keeps going.
- Standing eye level with the people around you. No stooping over a rollator, no looking up from a wheelchair. Conversations happen at everyone else's height.
- A tool that does not look like a medical device. The bright yellow bike reads as a bike. People see your face before they see a diagnosis.
- A community of more than 6,500 riders. Across four continents, organized around the #keepmoving hashtag, supporting each other online and at meetups. You do not ride one alone.
- A bigger world. It brings back the block you stopped walking to, the market you stopped visiting, and the reasons to head out the door, because getting back out is the whole idea.
Section SevenThree Ways To Get An Alinker
The Alinker comes in three sizes. The right size is set by inseam, not height.
Find your size in seconds
Move the slider to your inseam and we will point you to the right size.
Prefer the full reference? Here are all three sizes.
| Size | Minimum Inseam |
|---|---|
| Happy Small | 22" |
| Small | 27" |
| Medium | 32" |
If you are unsure of your size or between two of them, our team will walk you through the fitting process before any commitment is made. There are three ways to get an Alinker into your hands.
Buy it outright
Full payment, with shipping in roughly two to three weeks from the US warehouse.
Our 0% rent-to-own program
For riders who would rather spread the cost across paychecks or disability income, we run our own 0% interest rent-to-own program. A small deposit gets you started, and the balance is paid over eight months.
Community crowdfunding
For riders who cannot afford the bike outright, our community runs crowdfunding campaigns on behalf of individual riders. It is often topped up by other riders who already have one. This is how many of our riders got started.

The plateau is not the finish line.
Keep moving. That is what the Alinker is for.
Recovery after a stroke does not have to end when the appointments do. The research is clear that movement matters, and for the people the Alinker fits, it is a way to keep moving, keep getting out, and keep your world from shrinking. If you can still take a few steps, it may be worth a look.